What you’ll learn:
- How critical band aligned frequency allocation supports natural auditory processing.
- ECochG data shows high-performing traditional CI recipients align with functional auditory principles rather than anatomical assumptions.
- Evidence supports optimized performance using validated frequency allocation approaches for traditional CI candidates.
The Foundation of Traditional Place-Frequency Functions
This article provides evidence-based guidance on frequency allocation table (FAT) selection for traditional cochlear implant candidates with bilateral severe to profound sensorineural hearing loss. The recommendations presented here are grounded in decades of outcomes research and recent electrocochleography (ECochG) data demonstrating correlation between critical band aligned FATs and high-performance outcomes in this population.
Determining optimal frequency allocation for cochlear implant recipients requires careful consideration of the scientific framework guiding programming decisions. Anatomical models based on traditional place-frequency functions offer one approach, mapping frequencies to electrode locations according to mathematical formulas derived from structural measurements of the cochlea.
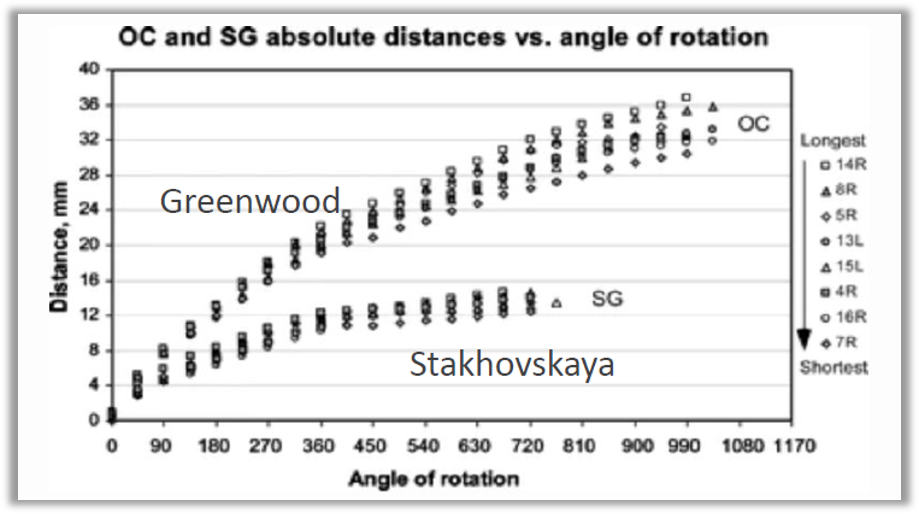
The Greenwood function originated from measurements in cadaver cochleae and animal models and estimates cochlear frequency based on the length of the Organ of Corti (OC)1, while Stakhovskaya’s work relied on anatomical measurements from temporal bone studies and maps frequency based on the position of spiral ganglion (SG) cells, which are typically present up to about 720 degrees in the cochlea2.
Furthermore, these models were developed using threshold measurements rather than suprathreshold responses. Cochlear implant users, however, experience sound at suprathreshold levels during everyday listening. This methodological mismatch means that the frequency representations derived from threshold data may not accurately reflect the perceptual experience of cochlear implant recipients during real-world communication.
Perhaps most importantly, these approaches do not account for elements of living cochleae such as fluid dynamics, membrane elasticity, activated outer hair cell function, and actual auditory nerve responses.3,4,5 No single mathematical formula can account for this biological diversity, yet traditional models apply uniform assumptions across all recipients. These limitations should challenge us to reconsider whether anatomical assumptions should drive frequency allocation decisions in current cochlear implant practice.
Critical Band Theory
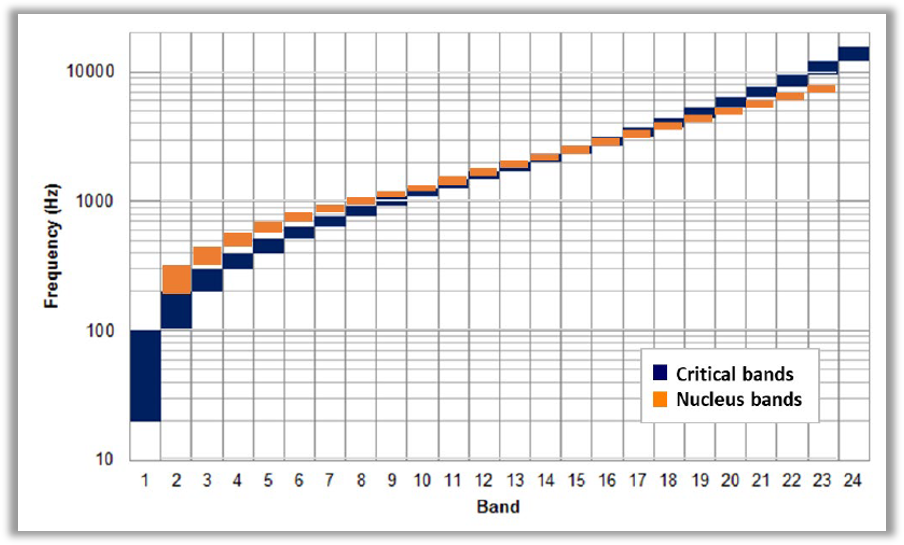
Beyond individual anatomical considerations, the broader question of how frequency information should be allocated across electrodes requires consideration of auditory perception principles. Critical band theory, established through decades of psychoacoustic research and serving as the basis for Cochlear’s Frequency Allocation Tables (FAT), describes how the auditory system naturally organizes frequency information into perceptually meaningful segments. The Nucleus Frequency Allocation Table is designed to approximate the selectivity of normal hearing within the frequency bandwidth of 188 to 7939 Hz distributed across 22 electrodes, allowing the frequency allocation to approximate the experimentally measured critical bands in humans.
Zwicker’s pioneering work on critical bands demonstrated that speech perception relies on these perceptual frequency groupings rather than on precise anatomical locations.6 By aligning frequency allocation tables with critical band relationships, we can leverage the auditory system’s natural processing mechanisms to facilitate more natural sound perception for cochlear implant users.
Evidence from Living Cochleae: ECochG Insights
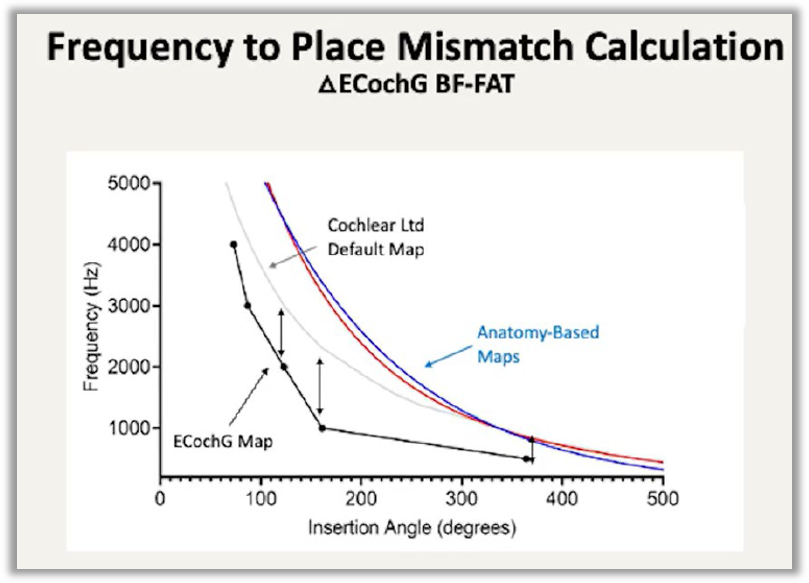
Recent advances in electrocochleography (ECochG) have enabled researchers to measure frequency responses from the living cochlea during cochlear implant surgery. These in vivo measurements from actual patients reveal a critical finding: the functional frequency-to-place relationship in living cochlear tissue demonstrates an approximate one-octave shift lower compared to predictions from traditional anatomical models7.
This consistent pattern across multiple patients suggests that anatomical measurements alone cannot capture the complex physiological reality of frequency processing in the living cochlea.
Research by Walia and colleagues (2024)8 using electrocochleography measurements during surgery has provided valuable insights into how the living cochlea organizes frequency information during real-world sound processing. Their data-driven mapping of cochlear frequency organization reveals important patterns that inform electrode design considerations. For lower frequencies between 500 Hz and 2 kHz, the average separation between frequency-specific sites along the cochlea spans approximately 75 degrees of cochlear angle. In contrast, higher frequencies from 2 to 4 kHz show much tighter spacing, with only about 22 degrees separating these frequency-specific regions.
This tighter clustering of high-frequency regions in the living cochlea has practical implications for electrode array design. When frequency-specific sites are more closely spaced, achieving adequate frequency resolution requires electrode contacts positioned close together to deliver appropriately distinct frequency information to these neighboring neural populations. Cochlear’s Slim Modiolar Electrode arrays are specifically engineered to address this need, featuring multiple closely spaced electrode contacts that can be positioned near the modiolus where spiral ganglion cells reside.
Clinical Performance Outcomes
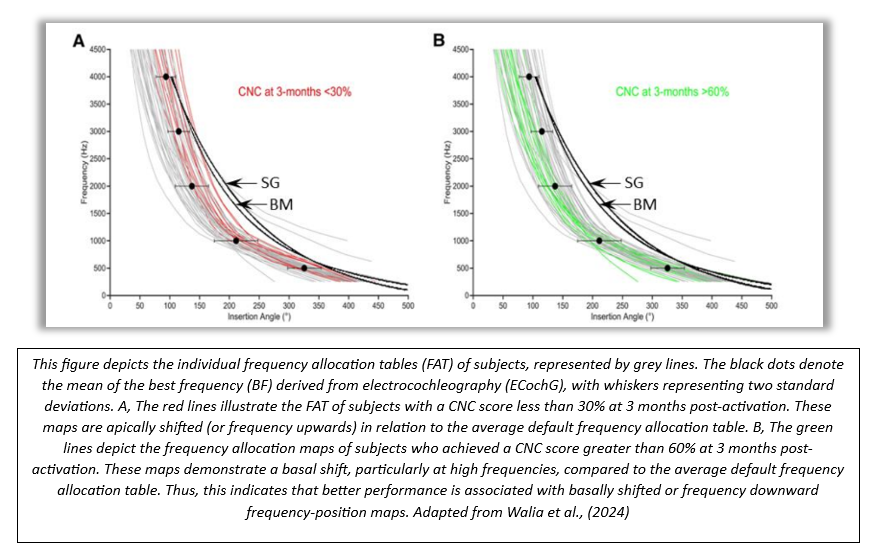
Clinical performance data for traditional CI candidates provides perhaps the most compelling evidence for the critical band approach. At three months after implantation, a CNC word score of 56% correct is considered the benchmark for speech perception performance.9 In a cohort of fifty adult CI recipients, Walia, et al. (2024)8 showed that the default FAT used by Nucleus CI recipients closely approximates the ECochG based frequency-place function. In the figure below, the red lines show the FATs for recipients who scored 30% or lower on CNC word tests at the same time point. In these poor performers, the FATs were oriented more towards traditional frequency-place functions and did not meet benchmark speech perception scores. The green lines show FATs for recipients who scored ≥60%. In contrast, these good performers had FATs oriented away from traditional frequency-place functions.
The research demonstrates that the functional approach to frequency allocation consistently correlates with superior performance outcomes compared to anatomical customization. This evidence base provides confidence that Cochlear’s critical band aligned default FAT represents an optimized starting point for acclimation in traditional candidates, grounded not in theoretical assumptions but in measured physiological responses and validated functional outcomes.
Clinical Implications for Modern Practice
The accumulating evidence suggests that cochlear implant frequency allocation should be guided primarily by validated perceptual principles and in vivo physiological measurements rather than relying exclusively on anatomical models developed from cadaver studies and animal models. Frequency allocation in Nucleus CIs is grounded in the concept of critical bands, developed through decades of foundational research into human auditory perception. The data validates what Cochlear’s critical band approach has assumed for decades: that functional performance in traditional recipients is optimized by frequency allocation that mirrors natural auditory processing mechanisms rather than anatomical assumptions based on cadaver studies or theoretical pitch place models.
Ultimately, speech perception outcomes are the most meaningful measure of benefit. As professionals, our responsibility is to base clinical decisions on the strongest available evidence while maintaining the flexibility to address individual patient needs. As cochlear implant candidacy has expanded, we now serve individuals with varying degrees of residual acoustic hearing through electric acoustic stimulation (EAS), patients with single sided deafness (SSD) seeking to restore binaural hearing, and recipients with unique anatomical or physiological characteristics that influence programming considerations. Each of these populations presents distinct clinical questions about frequency allocation, acoustic preservation, bimodal integration, and optimization strategies that deserve thorough exploration.
To learn more on how to optimize outcomes for individuals with single-sided deafness (SSD), stay tuned for next week’s article!
- Greenwood, D. D. (1990). A cochlear frequency-position function for several species—29 years later. Journal of the Acoustical Society of America, 87(6), 2592-2605. https://doi.org/10.1121/1.399052
- Stakhovskaya, O., Sridhar, D., Bonham, B. H., & Leake, P. A. (2007). Frequency map for the human cochlear spiral ganglion: Implications for cochlear implants. Journal of the Association for Research in Otolaryngology, 8(3), 220-233. https://doi.org/10.1007/s10162-007-0076-9
- Kemp, D. T. (1978). Stimulated acoustic emissions from within the human auditory system. Journal of the Acoustical Society of America, 64(5), 1386-1391. https://doi.org/10.1121/1.382104
- Rhode, W. S. (1978). Some observations on cochlear mechanics. Journal of the Acoustical Society of America, 64(1), 158-176. https://doi.org/10.1121/1.381981
- Brownell, W. E., Bader, C. R., Bertrand, D., & de Ribaupierre, Y. (1985). Evoked mechanical responses of isolated cochlear outer hair cells. Science, 227(4683), 194-196. https://doi.org/10.1126/science.3966153
- Zwicker, E. (1961). Subdivision of the audible frequency range into critical bands (Frequenzgruppen). Journal of the Acoustical Society of America, 33(2), 248. https://doi.org/10.1121/1.1908630
- Sagi, E., & Svirsky, M. A. (2025). A level-adjusted cochlear frequency-to-place map for estimating tonotopic frequency mismatch with a cochlear implant. Ear and Hearing, 46(4), 963-975. https://doi.org/10.1097/AUD.0000000000001641
- Walia, A., Shew, M. A., Varghese, J., Lefler, S. M., Bhat, A., Ortmann, A. J., Herzog, J. A., & Buchman, C. A. (2024). Electrocochleography-Based Tonotopic Map: II. Frequency-to-Place Mismatch Impacts Speech-Perception Outcomes in Cochlear Implant Recipients. Ear and hearing, 45(6), 1406–1417. https://doi.org/10.1097/AUD.0000000000001528
- Buchman CA, Herzog JA, McJunkin JL, et al. Assessment of Speech Understanding After Cochlear Implantation in Adult Hearing Aid Users: A Nonrandomized Controlled Trial. JAMA Otolaryngol Head Neck Surg. 2020;146(10):916–924. doi:10.1001/jamaoto.2020.1584
This material is intended for health professionals. If you are a consumer, please seek advice from your health professional about treatments for hearing loss. Outcomes may vary, and your health professional will advise you about the factors which could affect your outcome. Always read the instructions for use. Not all products are available in all countries. Please contact your local Cochlear representative for product information.
This blog is intended to serve as a resource for clinicians to help keep up to date with current clinical literature and is intended for professionals only. Clinical literature is based on research, which may include the experimental use of new or currently available products and technologies. Therefore, literature presented on this blog may represent use of Cochlear products that does not align with the intended use or indications approved by regulatory bodies, also known as off-label use. Cochlear does not condone any off-label use of its products, and it is not Cochlear’s intent to promote off-label use by providing this blog as a resource for healthcare professionals.
©Cochlear Limited 2026. All rights reserved. ACE, Advance Off-Stylet, AOS, Ardium, AutoNRT, Autosensitivity, Baha, Baha SoftWear, BCDrive, Beam, Bring Back the Beat, Button, Carina, Cochlear, 科利耳, コクレア, 코클리어, Cochlear SoftWear, Contour, コントゥア, Contour Advance, Custom Sound, DermaLock, Freedom, Hear now. And always, Hugfit, Human Design, Hybrid, Invisible Hearing, Kanso, LowPro, MET, MP3000, myCochlear, mySmartSound, NRT, Nucleus, Osia, Outcome Focused Fitting, Off-Stylet, Piezo Power, Profile, Slimline, SmartSound, Softip, SoundArc, SoundBand, True Wireless, the elliptical logo, Vistafix, Whisper, WindShield and Xidium are either trademarks or registered trademarks of the Cochlear group of companies.

