Morphometric Analysis and Linear Measurements of the Scala Tympani and Implications in Cochlear Implant Electrodes1
Fujiwara RJT, Ishiyama G, Lopez IA, Ishiyama A.
Research tells us that placement of an electrode within Scala tympani (ST) during cochlear implant surgery is desirable over placement in Scala vestibuli or a translocated array because it may lead to better performance outcomes.2,3 While we know placement in Scala tympani is desired, what about electrode positioning within that Scala? By analyzing the cross-section of 10 different electrode arrays as compared to the area of the ST at multiple points of insertion in human temporal bones, Fujiwara et al have shed new light on the impact on cochlea health in the delicate apical region.
Key Findings
- Scala tympani assumes an ovoid shape throughout the basal turn and, within the middle turn (360-450 degrees), develops into a triangular shape with its perimodiolar height greater than its lateral wall height.
- At >360 degrees, perimodiolar height (0.71mm Mean, 0.23mm SD) was significantly greater than lateral wall height (0.53mm Mean, 0.21mm SD). This trend continued towards the apex with lateral wall height decreasing at a faster rate than perimodiolar height.
- The changing shape of the Scala tympani in the apex may be more likely to lead to translocation, fibrosis or osteogenesis with electrodes with larger cross-sectional tip areas due to higher insertion forces required for complete insertion
- Increasing amounts of new bone formation have been positively correlated with a degree of intracochlear insertional trauma, which may lead to worsened postoperative audiological outcomes.
Discussion
The study analysis results suggest that an ideal scenario for avoiding trauma occurs when the electrode has the smallest possible tip volume measurement, avoids the basilar membrane and is not inserted past the point at which ST height becomes too shallow. Now why is this important as it translates to the overall health of the cochlea?
This ideal scenario can have a positive impact on cochlea health in several important ways. Impeding the basilar membrane’s function may negatively impact hearing performance which is important to avoid. The deeper the lateral wall insertion, the more likely the electrode will cause trauma1. Blood supply to the cochlea primarily lives within the lateral wall4, and lateral wall electrodes with larger cross-sectional tip volume may require increased insertion force. The impact on the lateral wall may introduce a blood supply resulting in increased immune response to that foreign body4,5,6.
The modelling of a fibrotic sheath or osteogenesis response demonstrates fibrosis or new bone growth around the electrode5. If the electrode is abutting the basilar membrane, the fibrotic sheath or bone growth may further impede its function4. The positioning of lateral wall electrode arrays results in fibrous tissue and new bone growth emerging between the electrode array and the spiral ganglion cells whereas this reaction occurs on the back side of perimodiolar electrode arrays. This reaction may be responsible for lower and more consistent impedances as well as reduced current levels required for stimulation on perimodiolar electrodes.7
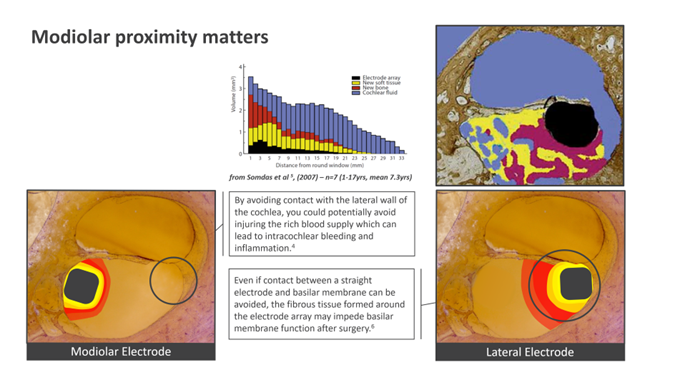
Fig 1. Re-modelling of the cochlea occurs after implantation which may negatively impact cochlea health. Peri-modiolar electrodes provide additional benefits promoting long term cochlea health by avoiding certain issues that impact lateral wall electrodes.
This analysis would indicate that best outcomes may be achieved with electrode arrays of smaller volume that avoid both the basilar membrane and the most apical region of the ST where it is most shallow. In the chart below1 we see that lateral wall vs Peri-modiolar height is similar up to about 180 degrees. Beyond that point however, the lateral wall height begins to decrease at a faster rate than perimodiolar height.
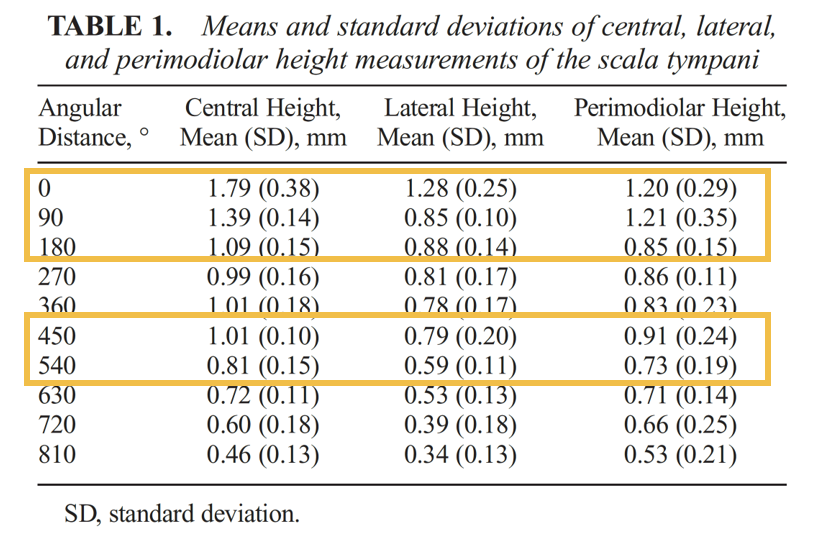
Table from Reference 1
Looking at the height of ST in a perimodiolar position, Cochlear™ Nucleus® electrodes are both positioned further away from the basilar membrane and have more tolerance for ST height to accommodate an atraumatic insertion. Specifically looking at the Slim Modiolar electrode, it’s mean cross sectional area of ST was 12.51% (SD, 2.78%) compared to other manufacturers electrodes with 22.34% (SD, 4.97%) for Midscala, and 32.16% (SD, 7.16% for Helix respectively. Among lateral wall electrodes, the CI622 occupies 7.82% (SD, 1.74%); FLEX24, 13.40% (SD, 2.98%); and SlimJ, 12.78% (SD, 2.84%).
Avoiding trauma during cochlear implantation helps promote long term hearing outcomes through structural preservation. Further minimizing the impacts of implanting a foreign body into the cochlea can provide long term benefits over the patient’s lifetime. The Slim Modiolar electrode not only offers performance benefits over lateral wall electrodes7, but the unique design offers the additional benefit of providing an atraumatic insertion to further promote the long-term health of the cochlea.
The impact on cochlea health is critical to a lifetime of hearing performance. Visit our website to explore additional data on outcomes with the Cochlear Nucleus System.
References:
- Fujiwara RJT, Ishiyama G, Lopez IA, Ishiyama A. Morphometric Analysis and Linear Measurements of the Scala Tympani and Implications in Cochlear Implant Electrodes. Otol Neurotol. 2023 Mar 8. doi: 10.1097/MAO.0000000000003848. Epub ahead of print. PMID: 36893208.
- Holden L, et al. Factors Affecting Open-Set Word Recognition in Adults With Cochlear Implants. Ear & Hearing. 2013;34(3):342-360
- Shaul C, et al. Scalar localisation of peri-modiolar electrodes and speech perception outcomes. The Journal of Laryngology & Otology. 2018;132(11):1000-1006.
- Bester C, et al. Four-point impedance as a biomarker for bleeding during cochlear implantation. Scientific Reports. 2020;10(1).
- Somdas M, et al. Quantitative Evaluation of New Bone and Fibrous Tissue in the Cochlea following Cochlear Implantation in the Human. Audiology and Neurotology. 2007;12(5):277-284.
- Verberne J, et al. The Effect of Scala Tympani Morphology on Basilar Membrane Contact With a Straight Electrode Array: A Human Temporal Bone Study. Otol Neurotol. 2017 Jan;38(1):47-53.
- Holder JT, et. al. Matched Cohort Comparison Indicates Superiority of Precurved Electrode Arrays. Otol Neurotol. 2019 Oct;40(9):1160-1166.

