- Approximately 5 minutes to read
- Learning objectives:
- Understand the importance of pitch matching
- Understand benefits of a perimodiolar array in pitch matching
- Gain practical programming tips to optimize hearing
Pitch matching between ears is an important aspect of our auditory system, enhancing our ability to interact with and interpret our environment effectively.¹ In the realm of cochlear implants, this topic has gained significant attention, particularly for individuals with single-sided deafness (SSD), or traditional bilateral or bimodal cochlear implant (CI) recipients who might compare their electric hearing to acoustic hearing on the contralateral side. This article will review key considerations for electrode selection, as well as straightforward programming tips to improve sound quality and the auditory experience for your Nucleus® System recipients if pitch mismatch is reported – no additional imaging required!
Start with Optimal Placement
Advancements in cochlear implant technology, particularly Cochlear’s perimodiolar electrodes, demonstrate a proven advantage of closer proximity to spiral ganglion cells, resulting in more focused stimulation of neural elements and improved speech perception.² In addition to this, perimodiolar arrays achieve equivalent spiral ganglion coverage compared to longer lateral wall arrays.³ Recent studies have also demonstrated that perimodiolar arrays significantly reduce mismatch compared to lateral wall arrays, making this an important consideration during electrode selection.4 This closer positioning not only enhances the precision of auditory stimulation but also contributes to a more natural hearing experience for users. Furthermore, the reduced mismatch can lead to better overall outcomes, highlighting the critical role of electrode design in cochlear implant performance.
Effortless Frequency Adjustments Without Imaging
Although pitch mismatch may be reduced with perimodiolar arrays, some level of tonotopic reorganization will naturally occur helping to overcome and adjust for place-pitch differences over time.5 However, this neural plasticity may not suffice for all patients, as some require additional programming adjustments to optimize their hearing and overall satisfaction. In these cases, pitch differences between ears can often be addressed through simple modifications of the Frequency Allocation Table (FAT) within Custom Sound® Pro™. To optimize sound quality, clinicians might trial MAPs with alternate low frequency cut-offs (188 Hz, 438 Hz, and 563 Hz) at initial activation or if significant pitch mismatch is reported. Encouraging patients to try MAPs with alternate FAT settings helps to determine preferred settings before their first follow-up visit and can improve sound quality and performance. ¹,6,7
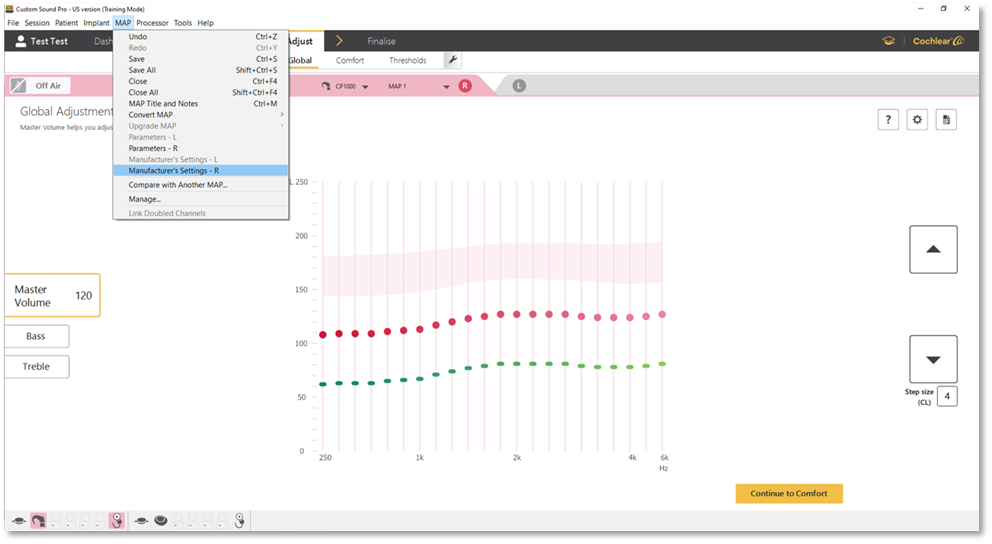
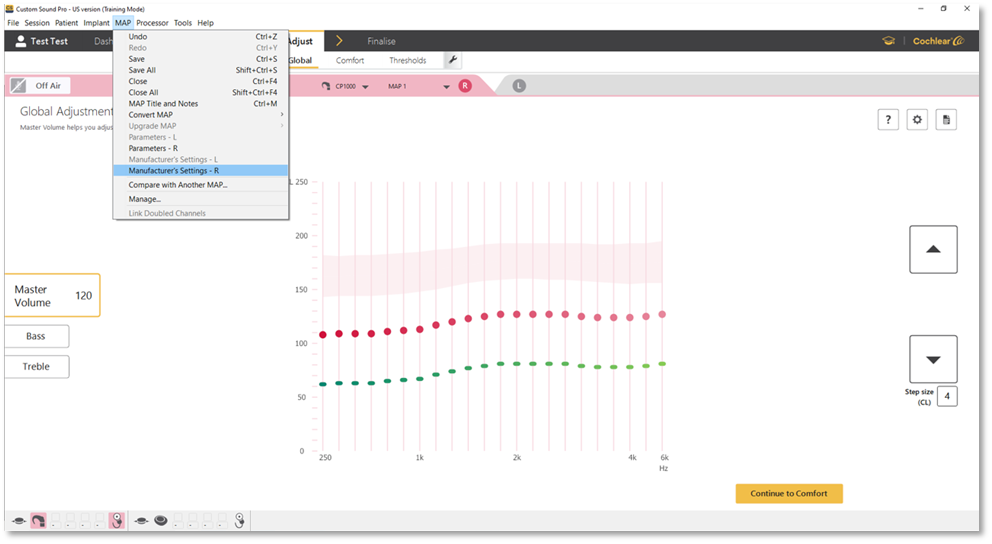
To access the FAT settings, navigate to the “MAP” tab in Custom Sound Pro, then select “Manufacturer’s Settings.”
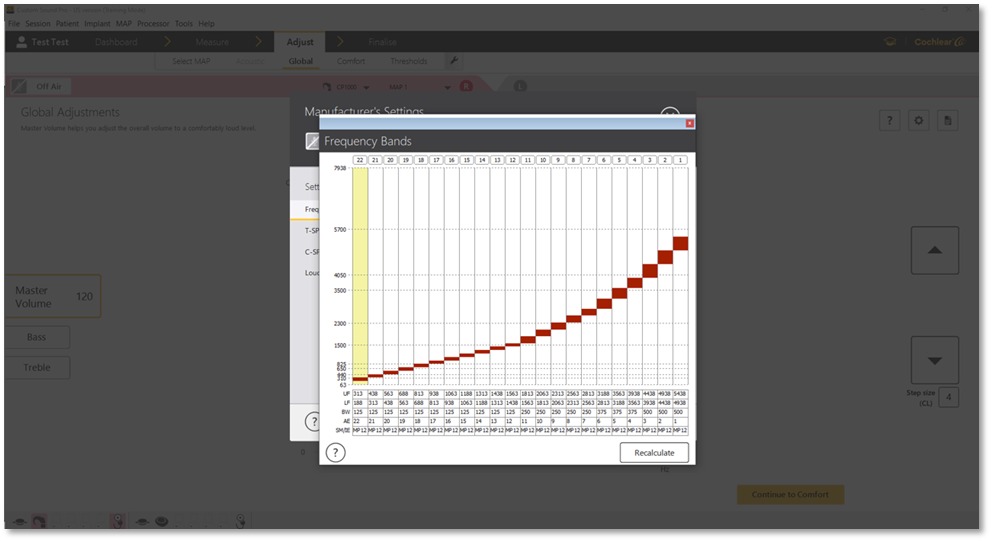
Next, select “Frequency Table” and choose a frequency range:
To view the frequency table, click on the 3 ellipses:
Conclusion
Advances in cochlear implant technology coupled with natural tonotopic reorganization and simple adjustments to frequency allocation have made it possible to achieve better pitch matching for Nucleus Cochlear Implant recipients.4,5,6,7 By leveraging these technological advancements and simple programming techniques, clinicians can better meet the unique needs of each patient, ultimately leading to more effective and satisfying hearing outcomes.
References
- Sagi E, Azadpour M, Neukam J, Capach NH, Svirsky MA. Reducing interaural tonotopic mismatch preserves binaural unmasking in cochlear implant simulations of single-sided deafness. Journal of the Acoustical Society of America. 2021;150(4):2316-2326.
- Holden LK, Finley CC, Firszt JB, Holden TA, Brenner C, Potts LG, et al. Factors affecting open-set word recognition in adults with cochlear implants. Ear Hear. 2013 May-Jun; 34(3):342–60.
- Danielian A, Ishiyama G, Lopez IA, Ishiyama A. Morphometric linear and angular measurements of the human cochlea in implant patients using 3-dimensional reconstruction. Hear Res. 2020 Feb;386:107874. doi: 10.1016/j.heares.2019.107874. Epub 2019 Dec 20. PMID: 31893539; PMCID: PMC7100312.
- Peters JPM, Bennink E, van Zanten GA. Comparison of Place-versus-Pitch Mismatch between a Perimodiolar and Lateral Wall Cochlear Implant Electrode Array in Patients with Single-Sided Deafness and a Cochlear Implant. Audiol Neurotol Neurotology. 2019; 24:28-48.
- Eggermont JJ. Acquired hearing loss and brain plasticity. Hear Res. 2017 Jan;343:176–90.
- Landsberger DM, Svrakic M, Roland JT Jr, Svirsky M. The Relationship Between Insertion Angles, Default Frequency Allocations, and Spiral Ganglion Place Pitch in Cochlear Implants. Ear Hear. 2015 Sep-Oct;36(5):e207–13.
- Tóth, TH, Németh, A, Bakó, P, Révész, P, Gerlinger, I, Szanyi I. (2023). Matching the pitch perception of the cochlear implanted ear with the contralateral ear in patients with sing-sided deafness: a novel approach. European Archives of Oto-Rhino-Laryngology. 280:4851-4859.

